

Recurrent Laryngeal Nerve (RLN) EMG Monitoring during Cervical Spine Surgeries
October 30, 2019
Faisal R. Jahangiri, M.D., CNIM, D.ABNM, FASNM, FASET1, Eloise Faust, CNIM1
1Axis Neuromonitoring LLC, Richardson, TX, USA;
A 33-year-old female with a history of bilateral arm pain, left arm numbness/tingling, and neck pain was admitted with cervical disc displacement and radiculopathy.
Magnetic Resonance Imaging (MRI) of the patient showed a C5-C6 mild left disc bulge causing mild to moderate compression on the C6 nerve root. Cervical X-ray revealed no dynamic instability. Pre-operative electromyogram (EMG) studies demonstrated a left C6 cervical radiculopathy. The surgeon decided to proceed with a one-level anterior cervical discectomy and fusion (ACDF) procedure at the C-C6 level to treat the herniated cervical disc.
A multimodality Intraoperative Neurophysiological Monitoring (IONM) protocol was planned to include bilateral median nerve, ulnar nerve and posterior tibial nerve Somatosensory Evoked Potentials (SSEPs) [1], bilateral upper and lower limb Transcranial electrical Motor Evoked Potentials (TCeMEPs), bilateral upper extremity EMG and Train of Four (TOF). The Recurrent Laryngeal Nerve (RLN) EMG was also included to prevent any RLN palsies, which has been previously reported in the literature during anterior cervical spine surgeries [2].
The procedure was performed by a fellowship-trained orthopedic spine surgeon, with a CNIM [3] certified technologist providing the neuromonitoring in the operating room, and a D.ABNM [4] board-certified neurophysiologist available via remote-monitoring. A board-certified neurologist with a specialty in IONM was also present online for remote monitoring during the entire surgical procedure [5].
During the surgical procedure, there was an EMG activity noted in the left recurrent laryngeal nerve after the surgeon placed the retractors (Figure 1). The surgeon was immediately alerted of the RLN irritation and activity. The surgeon readjusted the retractors to remove the pressure on the nerve, resulting in EMG returning to the baseline quite mode (Figure 2).
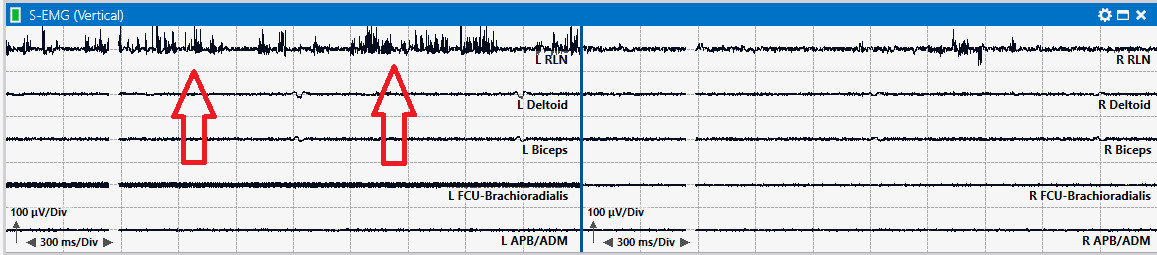
Figure 1: Abnormal EMG activity in the left recurrent laryngeal nerve recorded during an anterior cervical discectomy and fusion surgery.

Figure 2: EMG returned to baseline in the left recurrent laryngeal nerve after readjusting the retractors.
There was a change in RLN EMG during the procedure with no changes in SSEP or TCeMEP. The surgeon was immediately informed, and he released the retractors, and the EMG came back to baselines within a few minutes. Postoperatively, the patient had no neurological deficits due to early identification of EMG changes as well as quick intervention.
Damage to the RLN during the anterior cervical procedure has been reported in the literature, which may result in vocal cord paralysis, hoarseness, and dysphagia. The injury may result either due to direct sectioning or indirect compression. The common cause of indirect injury is retraction and compression [6].
References
| [1] | American Clinical Neurophysiological Society. "https://www.acns.org/pdf/guidelines/Guideline-11B.pdf." 2009. ACNS. Guideline 11B: Recommended standards for intraoperative monitoring of somatosensory evoked potentials. 29 May 2019. <https://www.acns.org/pdf/guidelines/Guideline-11B.pdf>. |
| [2] | Apfelbaum, RI, MD Kriskovich and JR Haller. "On the incidence, cause, and prevention of recurrent laryngeal nerve palsies during anterior cervical spine surgery." Spine (Phila Pa 1976) 25.22 (2000): 2906-12. |
|
[3] |
ABRET Neurodiagnostic Credentialing and Accreditation. ABRET. 9 Sep 2019. 9 Sep 2019. <https://www.abret.org/candidates/credentials/cnim/>. |
|
[4] |
ABNM: American Board of Neurophysiologic Monitoring. ABNM: American Board of Neurophysiologic Monitoring. 9 Sep 2019. 9 Sep 2019. <http://www.abnm.info/>. |
|
[5] |
Gertsch JH, Moreira JJ, Lee GR, Hastings JD, Ritzl E, Eccher MA, Cohen BA, Shils JL, McCaffrey MT, Balzer GK, Balzer JR, Boucharel W, Guo L, Hanson LL, Hemmer LB, Jahangiri FR, Mendez Vigil JA, Vogel RW, Wierzbowski LR, Wilent WB, Zuccaro JS, Yingling CD; membership of the ASNM. Practice guidelines for the supervising professional: intraoperative neurophysiological monitoring. J Clin Monit Comput. 2019 Apr;33(2):175-183. doi: 10.1007/s10877-018-0201-9. Epub 2018 Oct 30. |
|
[6] |
Erwood MS, Hadley MN, Gordon AS, Carroll WR, Agee BS, Walters BC. Recurrent laryngeal nerve injury following reoperative anterior cervical discectomy and fusion: a meta-analysis. J Neurosurg Spine. 2016 Aug 25(2):198-204. doi: 10.3171/2015.9.SPINE15187. Epub 2016 Mar 25. |